Analysis: How Medicaid Can Help Schools Support Students’ Mental Health
Easier to access Medicaid could sustain school-based mental health supports for students even after COVID relief funding runs out


;)
Untangle Your Mind!
Sign up for our free newsletter and start your day with in-depth reporting on the latest topics in education.
Education is at a Crossroads: Help Us Illuminate the Path Forward. Donate to The 74
A version of this essay appeared on the FutureEd website.
Among the COVID-19 pandemic’s most pernicious aftershocks is its impact on student mental health. Isolated at home, disconnected from friends and suffering trauma from family members’ job losses or pandemic-related deaths, students are experiencing high levels of anxiety and depression.
About 44% of adolescents experienced persistent feelings of sadness or hopelessness during the pandemic, compared with 37% in 2019, according to a recent survey by the Centers for Disease Control and Prevention. In schools, students’ struggles manifest as misbehavior, disengagement from classwork and spiraling absenteeism.
Recognizing this, districts across the country are using federal COVID relief aid to bring mental health professionals into schools and to expand social-emotional learning. Public schools have received nearly $190 billion in three waves of federal Elementary and Secondary School Emergency Relief (ESSER) funds that can be used for a range of priorities, including school-based mental health supports.
But this unprecedented infusion of federal aid also creates a challenge: how to sustain new school staff positions when the funding expires at the end of 2024. Medicaid, the federal-state partnership that provides health care for millions of public school students, could be part of the solution — as long as states take the necessary steps to use it and federal agencies back them up.
Drawing on a database of more than 4,400 local spending plans compiled by the data-services firm Burbio and covering 70% of the nation’s students, FutureEd found that more than a third of the local education agencies have earmarked a total of $1.2 billion in ESSER funding for psychologists, social workers and mental health counselors. If the trend continues, the investment could reach more than $2 billion.
Local jurisdictions range from California’s Poway Unified School District, which is earmarking nearly $10 million of its $17 million ESSER III allotment for hiring social workers, psychologists and counselors in its 38 schools, to the Hot Springs School District in Arkansas, which is spending $1.2 million of its $21 million allotment to employ therapists in some of its six schools.
Districts in nearly all states are making these investments, but the strategy is more popular in some states than others: 263 of the 583 California districts in the Burbio sample are planning to spend ESSER III funds on mental health professionals, compared with five of the 215 Arkansas districts in the sample.
Local investments also vary by geographic setting: 43% of districts and charters in cities and 41% of those in suburbs plan to spend on mental health workers, compared with 34% in small towns and 27% of rural districts, the analysis of the sample shows. This may reflect, in part, a lack of counselors and psychologists in more remote communities. Even in urban settings, some schools report having difficulty finding the mental health workers they need to support students.
Investments also vary by community poverty rates. Dividing the school districts in the Burbio database into four quartiles, FutureEd found that 32% of the districts with the highest poverty levels plan to bring in mental health professionals, compared with 40% of the most affluent quartile. The analysis did not include charter schools, for which poverty information was not readily available. Taken together, these are distressing findings, given the critical need for mental health supports among students in rural communities and in low-income neighborhoods.
Still, the White House estimates that public schools have already seen a 65% increase in the number of social workers and a 17% jump in counselors in recent months, due in large part to the latest round of ESSER funding. To sustain that funding, states and school districts could leverage Medicaid to support mental health care for students through a variety of mechanisms, including school-based health centers and partnerships with community providers, such as under Georgia’s Apex program. However, for districts that have hired their own mental health professionals and plan to keep those positions after ESSER funds expire, school Medicaid programs could help fill the gap.
In 2014, the federal government opened up a new avenue for support when it reversed what’s known as the free care rule and allowed schools to seek Medicaid reimbursement for certain health services provided by school employees, including mental health counselors, for all students enrolled in Medicaid. Previous guidance limited reimbursement to services included in a student’s Individualized Education Plan or Individualized Family Service Plan under the Individuals with Disabilities Education Act.
In 2019, about 36% of school-aged children were enrolled in Medicaid and the Children’s Health Insurance Program, according to estimates by Georgetown University’s Center for Children and Families. That number is likely even higher today, given that about half of all children in the United States (40 million) were enrolled in one of these programs as of January 2022, the vast majority through Medicaid. Given this, allowing school districts to receive reimbursement for services delivered by mental health workers and other health providers on their payroll could go a long way to sustain school mental health services after ESSER funds expire.
But not every district has that option. Expanding reimbursement beyond Medicaid-enrolled students with IEPs requires state action, often by submitting a Medicaid State Plan Amendment for approval by the federal Centers for Medicare and Medicaid Services. In some cases, the state legislature must first sign off on the change.
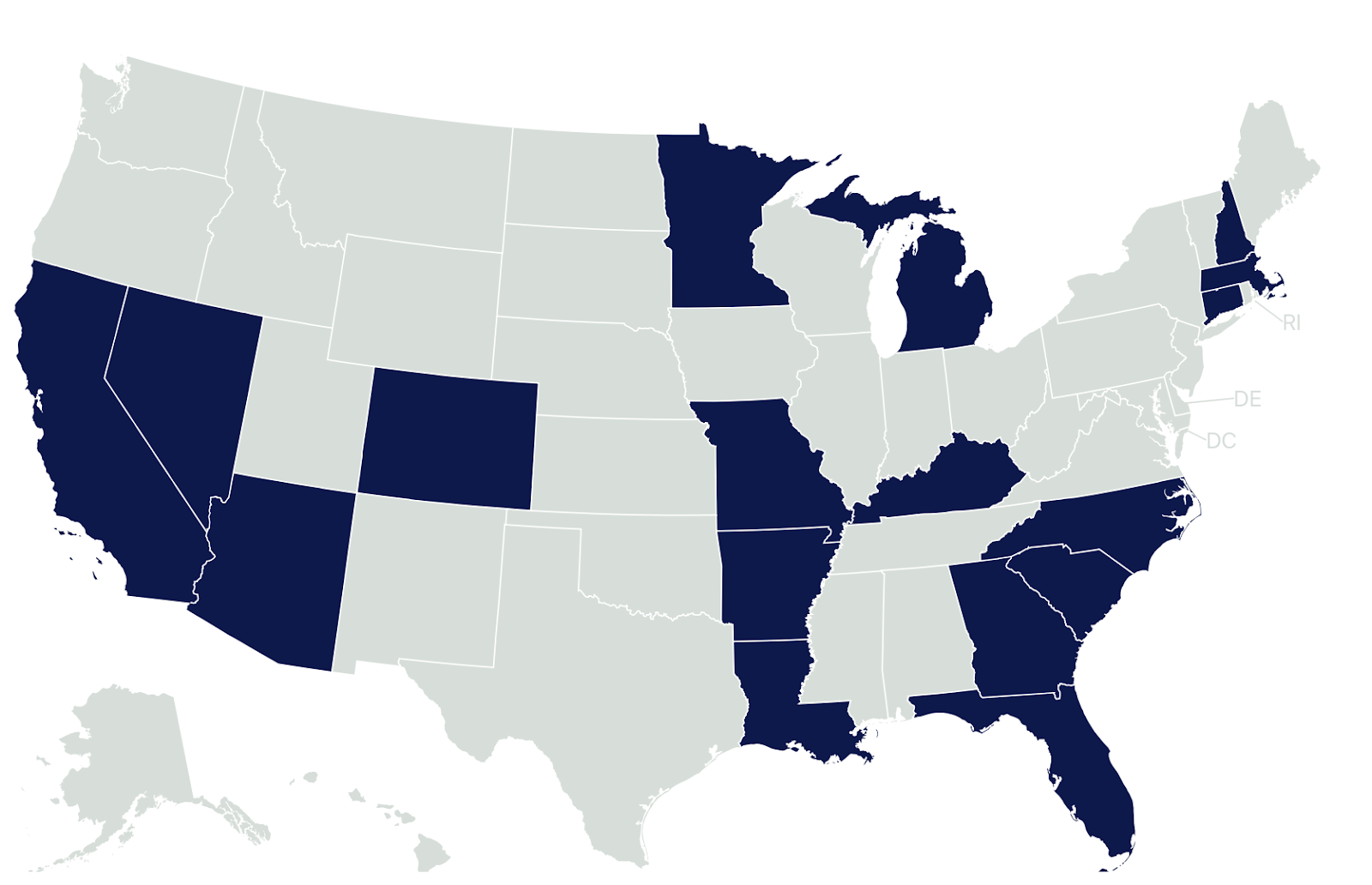
Currently, 16 states — Arkansas, Arizona, California, Colorado, Connecticut, Florida, Kentucky, Louisiana, Massachusetts, Michigan, Minnesota, Missouri, North Carolina, New Hampshire, Nevada and South Carolina — have expanded their programs to allow qualified school providers to bill for covered behavioral health services for Medicaid-enrolled students beyond those with IEPs, according to the Healthy Schools Campaign.
Connecticut limits the expansion to students with plans under Section 504, which are provided for some children with disabilities who don’t have IEPs. Georgia has also expanded its school Medicaid program but limits reimbursement to nursing services and thus was not included in this group for purposes of this analysis. Another five states — Illinois, Indiana, New Mexico, Oregon and Virginia — are expanding their programs but have not yet implemented them.
FutureEd’s analysis found that just over half of the 1,566 school districts and charter organizations in the Burbio sample that devoted federal ESSER funds to mental health professionals were in the states that have expanded their school Medicaid programs or are doing so. That means the other half that are investing ESSER III aid in mental health professionals are in states that do not allow broader reimbursement, and thus have limited options in using Medicaid to help sustain mental health staff on school payrolls once federal COVID relief aid expires.
Beyond necessary action, upcoming guidance from the federal Education Department and Department of Health and Human Services could make it easier to seek reimbursement for school-based mental health professionals. This could include an updated 2003 Medicaid school-based guide for how to submit administrative claims.
Such guidance could highlight opportunities for states to expand their school Medicaid programs under the free care reversal and provide claiming and billing information on topics such as parental consent and the alignment of licensure and provider requirements. Best practices for service delivery including the use of telehealth would also be helpful, as would strategies to address challenges to staffing school-based health services and making learning collaboratives and additional technical assistance available to states and school districts, especially for small and rural school districts with less capacity, so they can share successful strategies. This could also help districts, which face challenges in determining which providers are qualified for reimbursement and developing administrative tools and capacity for making claims.
Beyond these efforts, President Joe Biden’s fiscal year 2023 budget includes proposals to devote $1 billion for more school-based mental health professionals, including counselors, nurses, psychologists and social workers. The budget also supports a number of broader mental health initiatives, including $700 million in proposed funding for training, scholarships and loan repayment for providers willing to work in rural areas and other communities with limited access to services. And it includes more than $30 billion in Medicaid and mental health proposals, such as expanding access to certified community behavioral health clinics.
Congressional action would be required to move such proposals forward. Encouragingly, a number of congressional committees have announced bipartisan legislative efforts that include children’s mental health. Most recently, the House Energy and Commerce Committee drafted legislative language requiring HHS to issue guidance to state Medicaid agencies, elementary and secondary schools, and school-based health centers on reducing administrative barriers to providing health care services in schools.
Schools can serve as important partners in addressing students’ mental-health needs, especially if leaders make it easier to access school Medicaid programs. As the surgeon general noted in his recent advisory, addressing the youth mental health crisis is ultimately going to require a “whole-of-society” effort. Hopefully, the pandemic has made clear to educators, health care providers and society as a whole the importance of students’ mental and behavioral health to their academic success.
Phyllis W. Jordan is associate director of FutureEd, an independent, nonpartisan think tank at Georgetown University’s McCourt School of Public Policy. Anne Dwyer is an associate research professor of the practice at the Georgetown University McCourt School of Public Policy’s Center for Children and Families. Bella DiMarco is a policy analyst for FutureEd. Margaux Johnson-Green, a state health policy analyst with the Georgetown University Center for Children and Families, also contributed to this essay.
Get stories like these delivered straight to your inbox. Sign up for The 74 Newsletter
Phyllis W. Jordan is associate director of FutureEd, an independent, nonpartisan think tank at Georgetown University’s McCourt School of Public Policy.
contributors@the74million.org
Anne Dwyer is an associate research professor of the practice at the Georgetown University McCourt School of Public Policy’s Center for Children and Families.
contributors@the74million.orgBella DiMarco is a policy analyst for FutureEd. Prior to joining FutureEd, Bella worked at the Afterschool Alliance.
contributor@the74million.org